1 in 4 people has a flap-like hole in the heart – what can you do if you’re one of them?
Known as a patent foramen ovale, it is symptom-less and can potentially increase your risk of stroke – even if you don’t have high blood pressure or high cholesterol.
(Photo: iStock/tonefotografia)
Listen to this article
8 min
This audio is generated by an AI tool.
 Khoo Bee Khim
Khoo Bee Khim
17 Sep 2024 07:18AM (Updated: 17 Sep 2024 01:19PM)
17 Sep 2024 07:18AM (Updated: 17 Sep 2024 01:19PM)
There is a heart condition that is present in about
25 per cent of the population – or one in every four of the people you know. Some studies even place it higher at
27 per cent.
Unlike the chest pain, palpitations, lightheadedness or shortness of breath that coronary artery disease and heart failure can cause, this heart condition can lie undetected for years as there are no obvious symptoms – until you suffer a stroke like model
Hailey Bieber did in 2022 when she was just 25 years old.
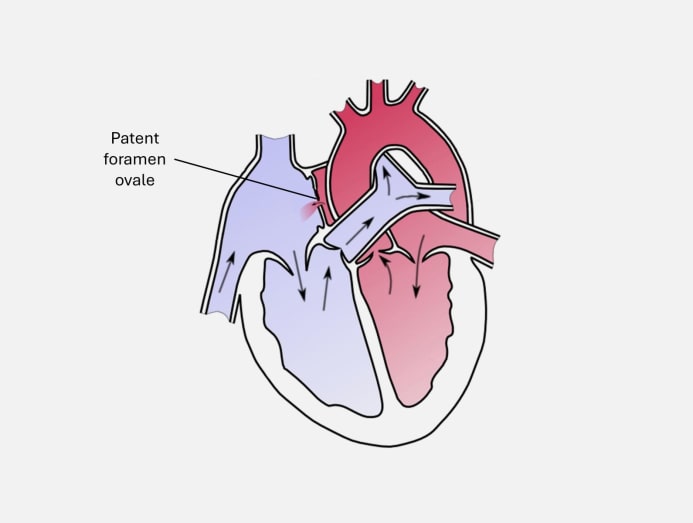
The condition is known as patent foramen ovale (PFO) and it takes the form of a small, flap-like hole in your heart that didn't close the way it should after birth. The small opening is located in the upper chambers – between the right and left atria – of the heart. In Bieber’s case, the hole in her heart measured between 12mm and 13mm.
“Normally, this opening closes due to changes in pressure within the heart after birth,” said Assistant Professor Foo Jie Sheng, a senior consultant with National Heart Centre Singapore’s (NHCS) Department of Cardiology and co-director of the Adult Congenital Heart Disease programme. "At NHCS, we see a wide range of patients with PFO, from as young as 17 to about 60 years old," he said.
(Art: Manco Capac/Wikimedia Commons)
In most people, this closing occurs spontaneously within two to three months of age, said Assistant Professor Ivandito Kuntjoro, the director of the Structural Heart Programme at National University Heart Centre, Singapore, and a senior consultant with the Department of Cardiology. Patients with PFO “will continue to have a persistent opening that allows blood flow to cross, especially when they cough or strain”, he said.
How does this small opening in the heart affect you if you have one? Here’s a look at how PFO is detected and treated.
WHAT CAN PFO LEAD TO?
A PFO “can potentially allow for the passage of blood clots from the right atrium to the left atrium, and into the rest of the body’s circulation”, said Asst Prof Foo.
Blood clots are not good news as they can get lodged in the blood vessels, and block or reduce blood supply. If one obstructs blood supply to the brain, it can cause an ischaemic stroke and prevent brain tissue from getting oxygen and nutrients. As a result, the affected brain cells will die in minutes.
However, “stroke associated with PFO is not the most common type of stroke”, said Asst Prof Kuntjoro, although it does affect “more young, fit patients” such as Bieber. These patients also do not have classic risk factors of stroke, he said, including smoking, or having high blood pressure or high cholesterol.
(Photo: iStock/Makhbubakhon Ismatova)
“Based on a National University Hospital study on stroke patients below 50 years of age, the definite cause of stroke cannot be found in 25 per cent of them. Among these 25 per cent, close to 40 per cent is found to have PFO,” said Asst Prof Kuntjoro.
Here are other issues that PFO has been associated with:
Some hormones such as serotonin can bypass the pulmonary circulation (the network of arteries and veins that exchange blood and other tissue fluids between the heart and lungs, and back) and pass directly through the blood-brain barrier to cause migraine, according to a study in
Journal Of Cardiology.
Emboli or tiny floating objects in your bloodstream such as a blood clot, an air bubble or a piece of fatty deposit can also pass through the PFO and find their way into a cerebral blood vessel. Instead of a stroke, an embolus can sometimes lead to a migraine attack. However, “the pathophysiological relationship and correlation between migraine and PFO is far from clear”, noted a study in
Frontiers.
- Decompression sickness (DCS)
“Decompression sickness is a big concern for those who scuba dive because when a diver re-surfaces, the release of nitrogen bubbles can cause a stroke if these bubbles cross the PFO,” said Asst Prof Foo.
The DCS risk in recreational divers has been reported at 3.6 cases per 10,000 dives, and a four-fold increase in risk with PFO, according to
Divers Alert Network. “The overall risk of neurological DCS is low, even in the presence of a PFO,” noted the website.
- Platypnea-orthodeoxia Syndrome (POS)
PFO can also lead to a rare condition known as platypnea-orthodeoxia syndrome, said Asst Prof Foo, “where a loss of oxygen saturation in the blood is observed” when you go from an upright to lying position.
HOW IS PFO USUALLY DETECTED SINCE THERE ARE NO SYMPTOMS?
According to Asst Prof Kuntjoro, “it is often discovered incidentally when a patient undergoes an echocardiography (an ultrasound of the heart), or CT coronary angiogram for other cardiac conditions”.
The diagnostic test to ask your doctor about, advised Asst Prof Foo, is the trans-oesophageal echocardiogram with bubble contrast. “It involves inserting a small tube with an ultrasound transducer on its tip down the throat to visualise the heart and inject tiny bubbles into the bloodstream to check for the presence of a PFO,” he said.
“A transcranial doppler is also a good screening test,” added Asst Prof Foo. “This test uses ultrasound to examine the blood flow in the brain and can help detect any bubbles that cross a PFO.”
(Photo: iStock/SARINYAPINNGAM)
Get yourself checked if you’ve had a stroke for which no obvious reason is found – and you’re under the age of 60. Although the number of PFO-related stroke cases is low in Singapore – for example, about 4 per cent or 310 cases out of 7,919 cases seen in 2021 – “the number of patients who underwent treatment in Singapore is at least four to five times lower than that estimate, signifying a potential group of patients who have yet to be diagnosed”, said Asst Prof Foo.
DOES PFO REQUIRE SURGERY?
The good news is, the majority of patients do
not need any treatment, said Asst Prof Kuntjoro. “If the PFO was deemed as the cause of paradoxical embolism (most commonly stroke), studies have shown that PFO closure, along with taking long-term blood thinners (such as aspirin), can reduce the recurrence of stroke,” he said.
If surgery is needed, it is commonly carried out “through a minimally invasive procedure known as a percutaneous closure”, said Asst Prof Kuntjoro. During this procedure, a catheter is inserted through the femoral vein in the leg and into the heart, said Asst Prof Foo. “A device is subsequently inserted through this catheter and left in the heart permanently to close the PFO,” he said.
(Photo: iStock/Pony Wang)
Asst Prof Kuntjoro noted that the procedure “can now be done under light sedation and the patient can return home the same day after observation in some cases”. “More complex cases may require general anaesthesia and a one-day stay in the hospital.”
The success rate of PFO device implantation is 96 per cent, said Asst Prof Foo. “Patients are typically required to take blood thinners for six months after the procedure to prevent blood clots from forming."
CAN PATIENTS EXERCISE?
If you have been diagnosed with a PFO before but have no symptoms, you can perform “normal exercises”, said Asst Prof Kuntjoro. But consider avoiding “scuba diving as it has been known to trigger decompression sickness and potentially, stroke”, he said. “For patients who have undergone a PFO device closure, they can resume regular exercise two to four weeks post-procedure.”
Generally, PFO patients should avoid the
valsalva manoeuvre, which is a breathing technique used in resistance training, lifting heavy loads and high intensity interval training”, said Asst Prof Foo. It is also used in scuba diving to open up blocked ears.
“The valsalva manoeuvre involves holding your breath while straining, which can increase right atrial pressure and hence, open the PFO,” said Asst Prof Foo.