- Joined
- Jan 5, 2010
- Messages
- 2,107
- Points
- 83
TTSH excuses itself for care lapse, says patient fell off the bed for his own good.
TTSH excuses itself for care lapse, says patient fell off the bed for his own good.
Me thinks that if TTSH is sued, it should be liable mostly if not totally for damages sustained as a result of the fall by Mr Teo in its ward in the night of 24Oct2011.
References (Published ST forum: 08Feb2012):
Patient falls after wife's request goes unheeded
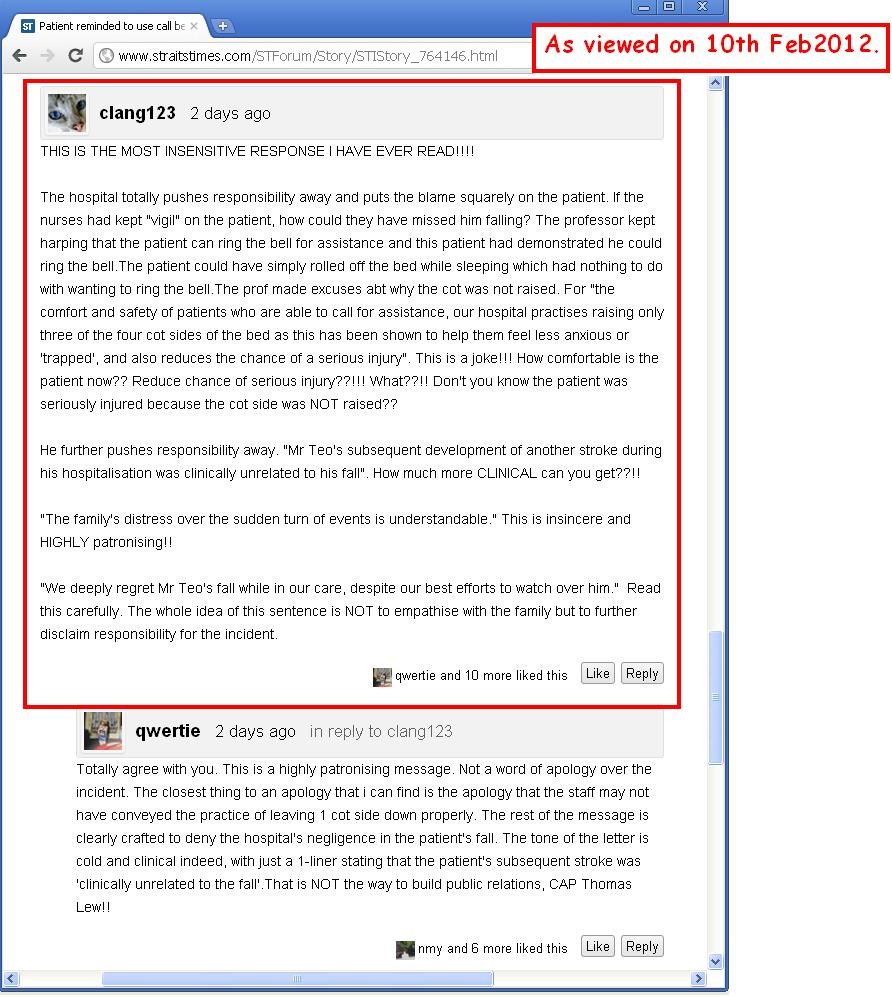
Patient reminded to use call bell if he needed help
 [img source]
[img source]
Reasons:
PS: As a side note, the Medical Board Chairman (TTSH) said "raising only three of the four cot sides of the bed as this has been shown to help them (patients) feel less anxious or 'trapped'": if the mindset of patients is so compromised such that they even feel 'trapped' in such a bed, then wouldn't more, rather than less nursing staff be needed deployed to care for these patients rather than excuses and lofty ideas about patient welfare be bandied around by professors? The implementation of fancy patient safety practices is no excuse for the lack of nursing staff on duty to care for patients at night.
The fact remains: the patient fell, hurt his spine and became paralyzed. Stressed by his condition, he suffered another stroke and is now totally disabled and bed-bound.
"An old man falling while in the care of a hospital shows lack of care." ~ how true is this statement.
Sometimes, the high GDP of Singapore has made it just economically not possible to say, yes we screw up and indeed we're sorry.

References:
TTSH excuses itself for care lapse, says patient fell off the bed for his own good.
Me thinks that if TTSH is sued, it should be liable mostly if not totally for damages sustained as a result of the fall by Mr Teo in its ward in the night of 24Oct2011.
References (Published ST forum: 08Feb2012):
Patient falls after wife's request goes unheeded
Patient reminded to use call bell if he needed help
Reasons:
- BOTH Family and hospital had noted the fall risk of the patient to be high.
- The family, by their judgement had explicitly asked the nurse to raise all 4 cot sides of the bed to prevent against the patient falling.
- The hospital refused/ ignored their request thinking that they knew better and insisted upon keeping the 4th cot side lowered.
- The fact that TTSH was aware of Ms Teo's father's "history of multiple strokes" meant that there would be a level of fragility and uncertainty regarding his behavior. The hospital was thus presumptuous to assume that since "Mr Teo had consistently demonstrated the ability to call for nurses' assistance via the call bell at his bedside" that there would be little chance of Mr Teo attempting to get up without sounding the call button- a repeat stroke/ delirium being of increased probability in Mr Teo's case.
- Whilst "raising only three of the four cot sides of the bed as this has been shown to help them feel less anxious or 'trapped', and also reduces the chance of a serious injury should they attempt to get down from the bed unassisted", another key feature of falls prevention should be the direct supervision of patients at all times of the day; and it was this important feature that the TTSH high fall-risk ward lacked.
- That said, it remains to be elucidate whether Prof Lew's quoted study was performed in the day or night or both. It would however be questionable what true impact the raising of the 4th cot side would have had on a sound-minded patient's psyche if the patient were bed-bound or aware that he had to call the nurse for assistance should he want to move- the nurse would be the one to lower the cot side in this case. Patients who"feel anxious or 'trapped'" by the mere presence of cot sides being up however cannot be defined as ordinary/ sound-minded patients and as such, greater care should be placed on their supervision and care. That falls from a bed with 4 cot sides up might be more serious that a bed with 3 cot sides up CANNOT be a valid excuse for the fall Mr Teo sustained in the said hospital as a result of short-handedness of nurses on duty that night.
- It might also be argued that but for the lowering of the 4th cot side, Mr Teo would not have fallen since the time taken for a patient to leave a bed with all sides up would obviously have been longer and more visible than the same scenario but from a bed with one cot side down. Given the described short duration during which Mr Teo sustained his fall, the nurse would have easily heard/ noticed Mr Teo's actions and taken immediate remedial action to prevent such a fall/ assist him as necessary. Keeping in mind that most of the ward patients would have been stroke patients of poor eyesight and senior age and possibly disorientated due to the night, more hospital staff should have been in attendance so that someone would always have a constant eye on all the patients, most of whom would have had 1 cot side down by inflexible hospital policy, and especially so in a 'high fall risk' cubical/ ward; an adequate staffing system should have been in place so that when one nurse attends to a patient, an assistant is present to watch over the patients, especially in a 'high fall risk' cubical/ ward.
- Notwithstanding the fact that the 4th cot side was down due to hospital policy, Mr Teo sustained his fall whilst in a 'high fall-risk' cubicle at TTSH. It would be the duty of the hospital as part of its care of the patient to ensure the safety and treatment of patients within its care. Mr Teo fell due to a lapse in the provision of care by the hospital and as a result of this lapse in care compounded by inflexible hospital policy and blatant disregard for the concerns/ suggestions of immediate relatives; other accessory comfort/ fall prevention measures notwithstanding.
- As a direct consequence of his fall that night, Mr Teo "sustained a cervical injury, which led to further weakness in his limbs" (Prof Lew) "and could no longer sit up or stand. He also could not eat or relieve himself unaided. He had to be fed blended food and had a catheter inserted.
For days after the incident, he was stressed and often delirious. A few days later, he had another stroke." (Ms teo)
PS: As a side note, the Medical Board Chairman (TTSH) said "raising only three of the four cot sides of the bed as this has been shown to help them (patients) feel less anxious or 'trapped'": if the mindset of patients is so compromised such that they even feel 'trapped' in such a bed, then wouldn't more, rather than less nursing staff be needed deployed to care for these patients rather than excuses and lofty ideas about patient welfare be bandied around by professors? The implementation of fancy patient safety practices is no excuse for the lack of nursing staff on duty to care for patients at night.
The fact remains: the patient fell, hurt his spine and became paralyzed. Stressed by his condition, he suffered another stroke and is now totally disabled and bed-bound.
"An old man falling while in the care of a hospital shows lack of care." ~ how true is this statement.
Sometimes, the high GDP of Singapore has made it just economically not possible to say, yes we screw up and indeed we're sorry.
References:
The Straits Times; Published on Feb 8, 2012
Patient falls after wife's request goes unheeded
MY 74-YEAR-OLD father was admitted to Tan Tock Seng Hospital after suffering an acute stroke last October. While he needed help to walk to the toilet, he could sit and eat by himself. However, he was placed in a 'high fall-risk' cubicle.
Subsequently, the ward doctor informed me that my father was in a stable condition and the hospital was planning to transfer him to Ren Ci Hospital for rehabilitation.
My mother visited him in the evening, and before leaving, she saw that one cot side was down. She reminded the nurse about it as she was afraid my father might attempt to leave the bed unassisted.
That night, my father fell from the cot. Apparently, the nurse on duty found him lying on the floor. The fall injured his spine. He suffered further weakness to his limbs and could no longer sit up or stand. He also could not eat or relieve himself unaided. He had to be fed blended food and had a catheter inserted.
For days after the incident, he was stressed and often delirious. A few days later, he had another stroke.
My father was in a high fall-risk ward. That meant the nurses on duty had to keep a close watch on all the patients there. Why was it that my father could attempt to leave the bed without anyone noticing it?
My mother reminded the nurse to raise the cot side before she left. But that was not done. If the staff had done as instructed, the accident would not have happened.
My father stayed in the hospital for 70 days. Today, he is totally disabled and bedridden as a result of the fall and consequent stroke. The fall should not have happened.
I am disheartened by the entire incident. An old man falling while in the care of a hospital shows lack of care.
Ivy Teo (Ms)
Patient falls after wife's request goes unheeded
The Straits Times; Published on Feb 8, 2012
Patient reminded to use call bell if he needed help
WE EMPATHISE with the condition of Ms Ivy Teo's father and the stress it creates for the family.
Her father has a history of multiple strokes. He was admitted to a ward with a designated 'high fall-risk' cubicle following an acute stroke.
There, our nurses keep vigil and provide frequent assistance to patients when they wish to move around, and render aid promptly whenever alarm devices such as the call bell are activated.
During his stay, Mr Teo had consistently demonstrated the ability to call for nurses' assistance via the call bell at his bedside.
On Oct 24, our nurses had, during their ward rounds, reminded Mr Teo to use the call bell if he needed assistance. Unfortunately, when our nurse was attending to an adjacent patient and had her back to him, Mr Teo fell. He was seen to immediately but sustained a cervical injury, which led to further weakness in his limbs. We understand Ms Teo's mother had earlier requested that the fourth cot side of the patient's bed be raised.
However, for the comfort and safety of patients who are able to call for assistance, our hospital practises raising only three of the four cot sides of the bed as this has been shown to help them feel less anxious or 'trapped', and also reduces the chance of a serious injury should they attempt to get down from the bed unassisted.
We apologise that our staff may not have conveyed the practice clearly to Mrs Teo.
Mr Teo's subsequent development of another stroke during his hospitalisation was clinically unrelated to his fall.
The family's distress over the sudden turn of events is understandable. We deeply regret Mr Teo's fall while in our care, despite our best efforts to watch over him.
Clinical Associate Professor Thomas Lew
Chairman, Medical Board
Tan Tock Seng Hospital
Patient reminded to use call bell if he needed help
Last edited: