- Joined
- Jul 10, 2008
- Messages
- 63,746
- Points
- 113
I went to look at the article from the Indian Dental Tribune that you mentioned. It's data is a bit older. Latest numbers are :
Parameter values Table 1
Parameter Scenario 1 Scenario 2 Scenario 3 Scenario 4 Scenario 5:
Current Best EstimateR0* 2.0 2.0 4.0 4.0 2.5 Infection Fatality Ratio, Overall† 0.005 0.005 0.008 0.008 0.0065 Percent of infections that are asymptomatic§ 10% 70% 10% 70% 40% Infectiousness of asymptomatic individuals relative to symptomatic¶ 25% 100% 25% 100% 75% Percentage of transmission occurring prior to symptom onset** 35% 70% 35% 70% 50%
Numbers are somewhat higher than mentioned in the report.
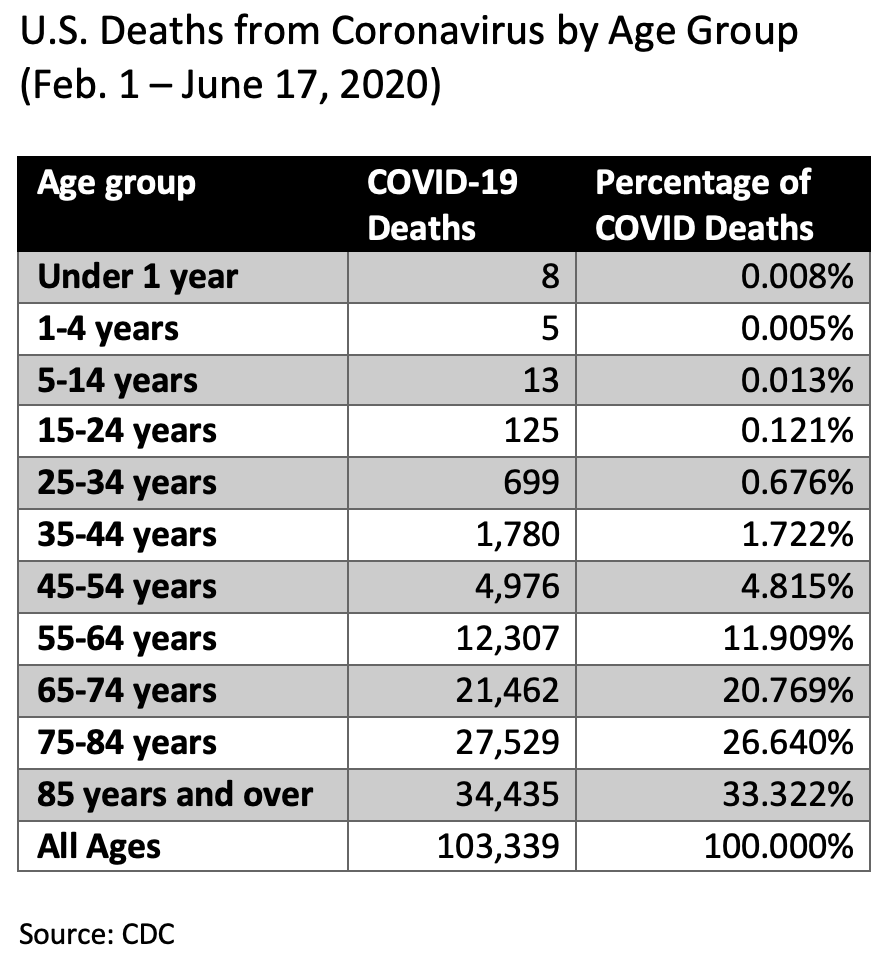
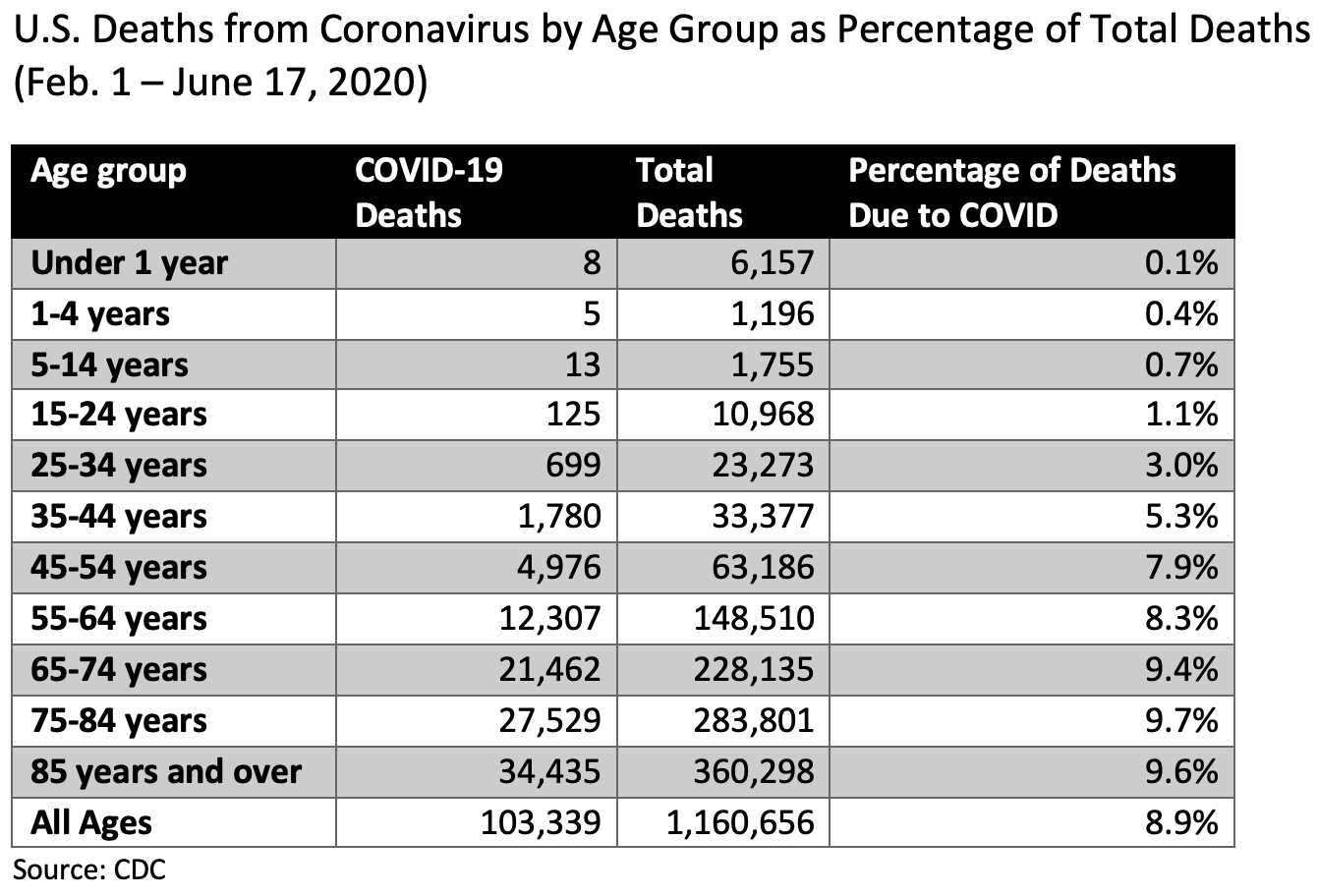
Regarding case vs infection fatality. Yes I agree case numbers are an estimate. It could go either way. Case fatality could be an underestimate because people are dropping dead without testing positive or it could be an overestimate because people are running around without showing symptoms at all. I don't know how or what testing coverage is like, but the CDC's own estimates arising from these infection rates are much higher than would be expected. I'm including it again for easy reference :
View attachment 87484
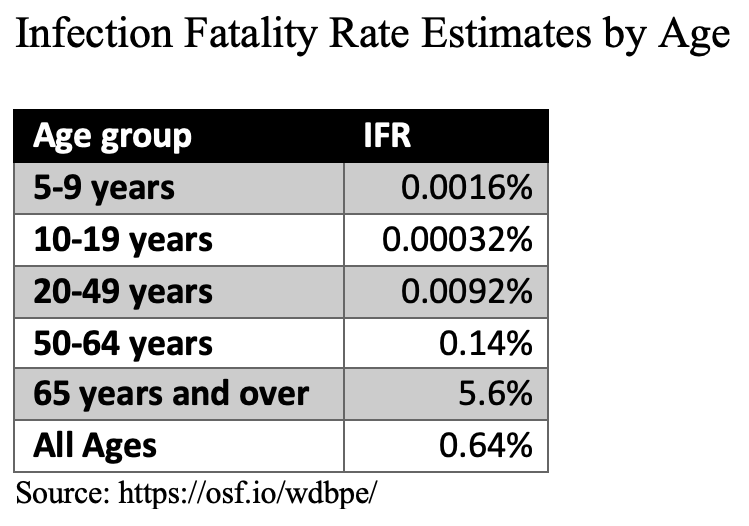
Please note that both the new IFR and this table reference data that supercedes the Indian dental tribune's data.
Assuming that the CDC is it's own best judge as to how they estimate their testing coverage, who am I to argue?
Nonetheless, your Indian dental tribune rebuttal has no comparative data with the flu virus and doesn't disprove the above chart. The data above is the CDC's own for both.
The numbers are similar. But the situation isn't. Your flu article sources excess WINTER deaths. We're not in winter yet where the flu is at it's peak. Rather the disease has hit just as spring has sprung (pardon the pun). I can't be sure, but I think you're comparing numbers for flu post-peak and Covid pre-peak. If that's the case, there's this old saw about counting chickens before they've hatched.
We're about the halfway mark for the year for this virus and you could approximately double the deaths assuming linear growth. However, we all know that diseases do not spread according to linear growth do we? If it follows geometric growth, we could be in a heap of more fatalities. Plus we will be going into winter.
Since we're pulling data from other sources, why not go straight to the end point. How we deal with dead bodies.
So far all sources indicate that institutions dealing with death are far busier than normal. And they attribute this to the virus.
https://www.theguardian.com/world/2...puts-pressure-on-crematoria-and-morgues-in-uk
https://www.nytimes.com/2020/04/02/nyregion/coronavirus-new-york-bodies.html
if death institutions are busier than normal, would that be the case every winter as well from the flu? you would think they would have raised capacity by now.
Well for now I advise caution and I certainly don't envy those who have to make decisions for the whole country without fully knowing how this virus behaves.
If you take Sweden to be representative of how the virus behaves it means that if the rest of the world had not mucked around with lockdowns most countries would be out of the woods already.
https://www.covid19insweden.com/en/
There have been no excess deaths in July 2020 in Sweden.
https://www.covid19insweden.com/en/deaths.html
Minimal social distancing, schools, cafes, shops remained open and no masks were required. Outside of Stockholm case numbers and mortality were on par with other Nordic countries that did lockdown.
Stockholm has the same problem as other big cities in Spain, Italy etc... ie too many you know whats which cannot be singled out for obvious reasons.